"Disease Prevention" suggests an intervention occurs PRIOR to disease manifesting. If screening methods only prompt intervention when a disease biomarker is present, what are we preventing?
Disease prevention has never mattered more. As America’s population ages, healthcare spending is poised to skyrocket—so bending the cost curve is no longer optional; it’s imperative. But even if we commit to keeping people healthy, do we actually have the tools to pull it off?
How do Screen for and Treat for Chronic Disease?
Chronic disease screening includes testing biomarkers for infectious diseases like HIV and Hepatitis C, blood pressure screening, cancer screening (e.g. imaging based or now cell-free DNA), depression screening, and type 2 diabetes. The frequency at which certain biomarkers are tested, and for what population, is recommended by different specialty organizations (like the American Heart Association, American College of Lifestyle Medicine, etc.) or most definitively by the US Preventive Services Task Force (USPSTF).
Regular screenings AND additional services, like “Healthy Diet and Physical Activity for Cardiovascular Disease Prevention in Adults With Cardiovascular Risk Factors” are listed in the USPSTF recommendations.
Importantly, all recommendations that are A&B rating of evidence from the USPSTF require, under the Affordable Care Act and federal code, from “group health plans and health insurance insurers offering non-grandfathered group or individual health insurance coverage provide coverage of certain specified preventive services without cost sharing.”
This is pretty cool. In theory, if the scientific evidence reviewed by a non-biased committee demonstrates a population level benefit, there is a universal code that guides the practice of medicine AND reimbursement strategy. However, the fundamental flaw is that these recommendations for disease “prevention” occur because the metrics we have available to us quantify disease presence, rather than signals prior to disease onset.
USPSTF Recommendation for Intervention Require Disease Biomarkers to Be Elevated
Let’s take behavioral interventions to prevent obesity-related morbidity and mortality in adults. In order to a diet and exercise intervention to be recommended, the USPSTF requires that the individual have a BMI >30 (which is treatable obesity), or a BMI >25 with hypertension, dyslipidemia, abnormal glucose levels, or diabetes.
If an intervention is suggested when the individual already has a classifiable disease, what are we preventing?
One could argue that we are preventing the long term complications (e.g. organ failure or death) indicated by the disease biomarkers.
To dive into this argument, the NIH funded diabetes prevention program (DPP) serves as an excellent case study, as this cohort was followed for >15 years following a randomization to an intensive lifestyle intervention, metformin, or placebo in patients with pre-diabetes.
Early Lifestyle or Metformin Interventions for Pre-Diabetes Were Associated with Lower Rates of Diabetes
The NIH funded DPP endeavored to decrease the rate of diabetes incidence by prescribing metformin or an intensive lifestyle change program (with a coach) to individuals with pre-diabetes (but not yet diabetes) using an A1C cut-off of 5.7%.
After 10 years they found that the cumulative incidence of diabetes was:
Lifestyle: 5 per 100 person years (42% cumulative incidence)
Metformin: 7.9 per 100 person years (47% cumulative incidence)
Placebo: 10.8 per 100 person years (52% cumulative incidence)
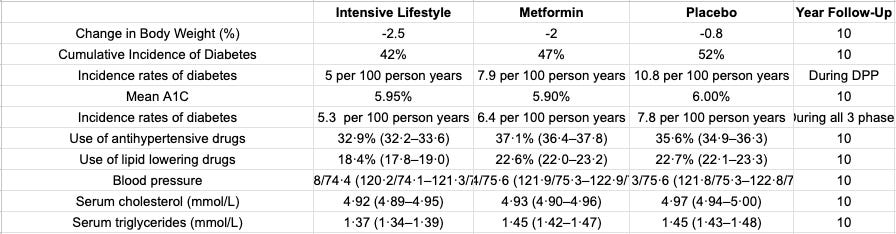
This demonstrated a success! Lifestyle (to a greater degree) and metformin when prescribed earlier were able to lower diabetes rates. Using A1C as the early indicator of diabetes risk, the goal of preventing diabetes diagnosis (compared to placebo) was achieved.
However, Early Metformin Did Not Prevent Long Term Organ Failure, While Lifestyle Did
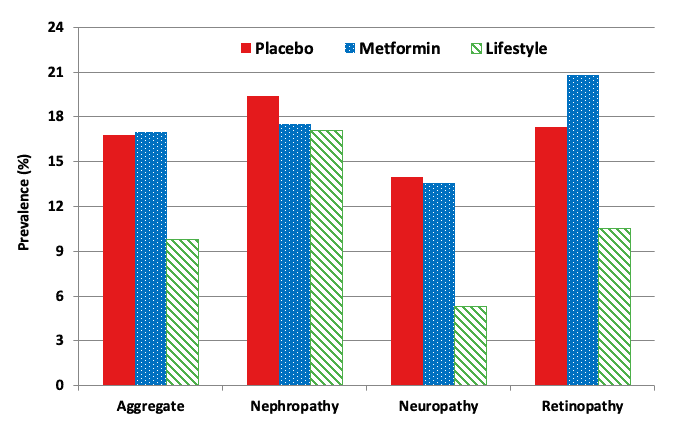
Microvascular complications over 15-year follow-up: the Diabetes Prevention Program Outcomes Study (Supplemental Table #3)
It is nice to not have a diagnosis of diabetes. But it is more important to have functioning organs as a result of not having this diagnosis. Some interesting findings we’re tucked away in the supplemental tables of the 15 year follow up from the diabetes prevention program.
“In a post-hoc analysis among those whose latest HbA1c was ≥6.5%, representing ~25% of the cohort, lifestyle showed significant reductions compared with placebo in the aggregate microvascular outcome (relative risk 0.59), retinopathy (relative risk 0.51), and neuropathy (relative risk 0.39), with no significant differences between the metformin and placebo groups.”
Even if identified “early,” what was first line therapy had no benefit on prevention of long term complications in the patients with the most elevated A1C.
While this doesn’t demonstrate an issue with disease screening, it demonstrates that our interventions are often tailored towards the wrong metrics (e.g. A1C). While yes it is good to not “have a diagnosis,” what is better is not having the long term complications. This is especially true for drugs that target a single molecular pathway in order to modify a single blood-based biomarker.
Early Prevention: What about the person with BMI 29, A1C 5.6%, Cholesterol 199, BP of 130/81?
Take a 44 year old man with the following metrics above. Their Framingham Risk 10 year is <5% and their PREVENT score is low risk. They do not meet current disease threshold criteria, and likely no intervention would be covered to prevent them from progressing to a quantifiable disease state.
If you were to examine their cardiovascular fitness, body composition (e.g. muscle mass index, body fat %, or visceral fat content), or insulin sensitivity, you would have a much fuller picture of their health status.
Let’s estimate his VO2max using a rough regression adjustment (Jackson et al. 1990) uses age and BMI yielding:
Plugging in 44 yrs and BMI 29:
This person’s estimated VO2max is in the bottom 10th percentile for men 40-49 from the FRIEND registry and below the 5th percentile from the Cooper Clinic (Mayo Clinic Proceedings 2015).
Rather than waiting for this individual to have a disease biomarker present, wouldn’t it make sense to focus on the low exercise capacity?
An intervention tailored not towards simply reversing a single disease biomarker, but towards improving fitness, body composition, and insulin sensitivity would improve their physical function AND prevent multi-morbidity disease & mortality risk.
Focus on Function, Rather than Presence of Disease
What if the biomarker panel measured the functions of the body, rather than signals that arise when the body can not longer compensate for nutrient overload or chronic stress?
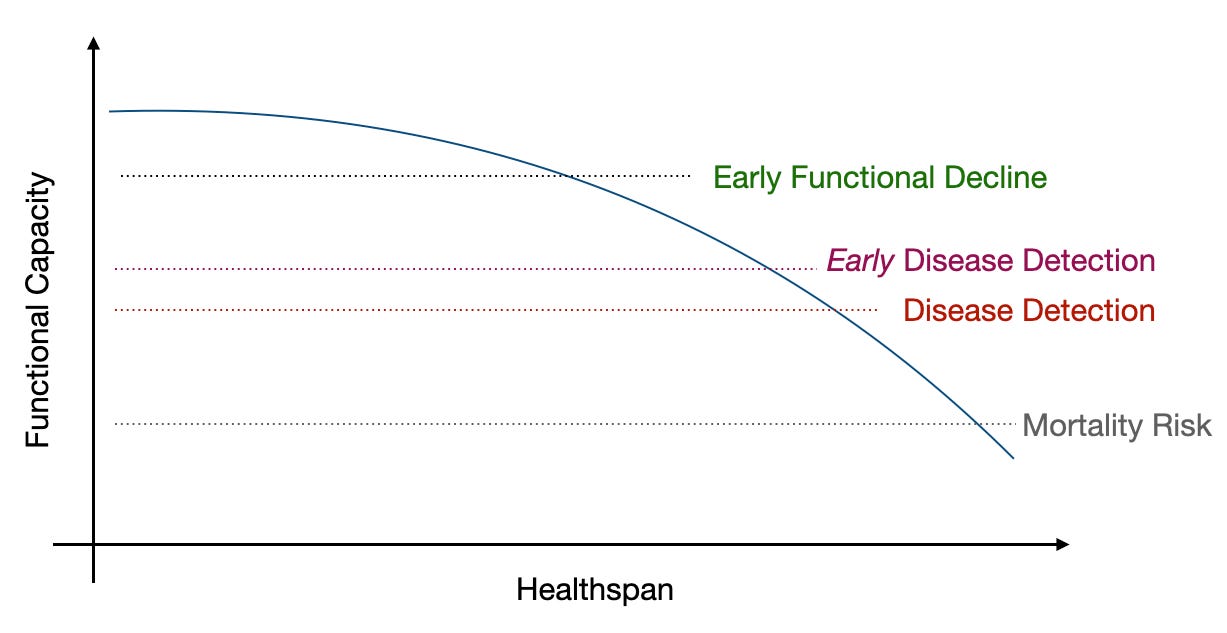
The current paradigm focuses on disease detection through population-based screening recommendations.
Direct to consumer health platforms (e.g. Function, Superpower, Mito, Everlywell, InsideTracker, etc.) provide disease detection biomarkers on demand, outside (or inside) of USPSTF recommendations. This may allow for early disease detection.
However, if we truly want preventive and proactive healthcare, we need to focus on the earliest declines in functional capacity. We would be able to capture, and act on, early functional decline.
Wouldn’t you want to understand that muscle quality is decreasing before frailty, or significant muscle loss, kicks in? Or that your cardiovascular system is on its way down, before you need to be started on a band-aid medication?
Focusing on biomarkers of cardiovascular function (like exercise capacity), body composition (visceral fat and muscle mass), and insulin sensitivity are key functional measures that can truly indicate health status, predict multi-morbidity, and do not require that our organ systems have been unable to compensate, resulting in disease biomarker presence.
Source: VO Health CEO Brooks Leitner's Substack: Read More Here

Written by
Brooks Leitner, MD PhD
Reading Time
8min